



A new global analysis has delivered a sobering message: despite two decades of medical progress, hypertension remains a runaway public‑health crisis — and the world is losing ground where it matters most.
The study, led by researchers at Tulane University and published in the Journal of the American College of Cardiology, shows that high blood pressure continues to rise sharply in low‑ and middle‑income countries, even as wealthier nations make only modest gains in control rates.
Hypertension is often described as the “silent epidemic,” and this report confirms just how silent — and how deadly — it remains.
Simple but complicated
Hypertension is, in theory, one of the simplest chronic conditions to diagnose and manage. Testing is quick, medications are widely available, and lifestyle interventions — from diet to physical activity — are well understood. Yet the global picture tells a different story.
The Tulane team found that hypertension now affects 1.7 billion adults worldwide, or 33% of the global adult population. It is the leading preventable cause of premature death, responsible for an estimated 10 million deaths every year
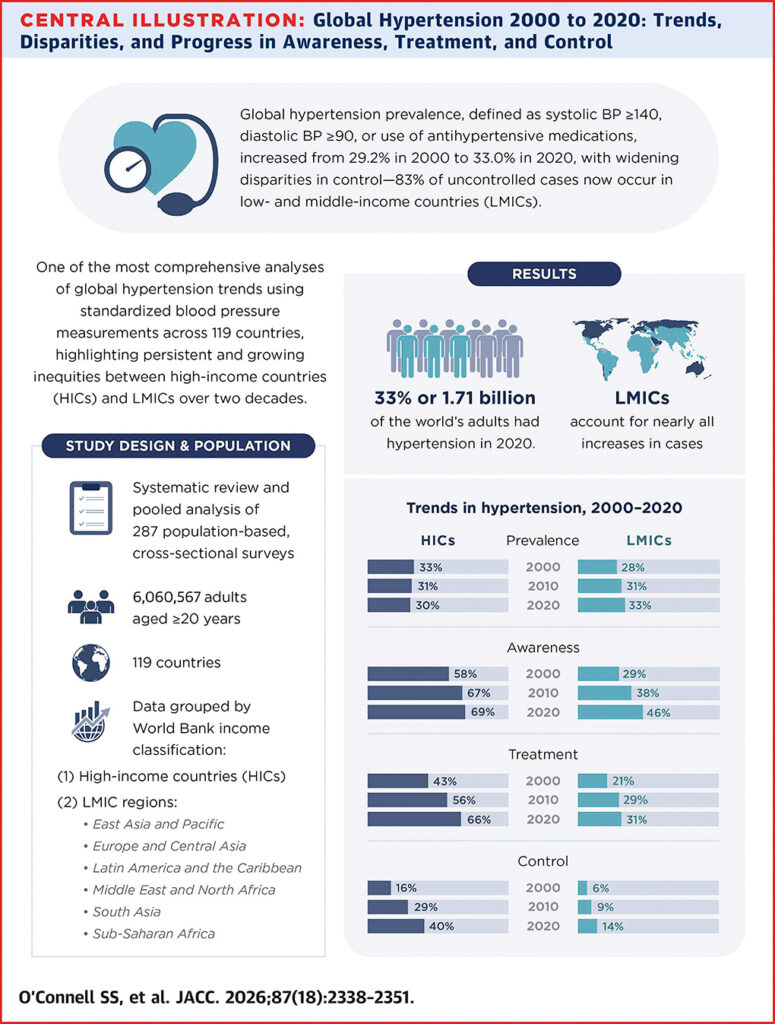
Despite this, fewer than 20% of adults with hypertension had their blood pressure under control in 2020.
Lead author Samantha O’Connell notes that the gaps are not confined to poorer nations. Awareness, treatment, and control “are not where they need to be… not only in low‑ and middle‑income countries but also in high‑income countries”.
Ninety per cent of the global increase is in lower‑income countries
The most striking finding is the widening global divide. From 2000 to 2020, hypertension prevalence decreased slightly in high‑income countries but rose substantially in low‑ and middle‑income countries
Nearly 90% of the global increase in adults with hypertension occurred in these lower‑income regions
By 2020, 83% of adults with uncontrolled hypertension lived in low‑ and middle‑income countries, up from 70% in 2000
These countries face a perfect storm:
- rapidly growing populations
- rising rates of obesity and sedentary lifestyles
- limited access to chronic‑disease care
- health systems still burdened by infectious diseases and maternal/child health needs
The result is a mounting crisis with enormous economic and social consequences.
High‑income countries underperforming
While wealthier nations fare better, the numbers are still far from reassuring. Hypertension control rates in high‑income countries sit at 40.2%, nearly three times higher than the 13.6% seen in low‑ and middle‑income countries — but still unacceptably low given the tools available.
Senior author Katherine Mills underscores the point: “Control is still only about 40% in high‑income countries, despite the fact that we have effective interventions”
The barriers are multilayered:
- Inconsistent adherence to treatment guidelines by clinicians
- medication access and affordability
- patient challenges with long‑term adherence
- difficulty sustaining lifestyle changes
- fragmented health systems that do not support chronic‑disease management
Where it hits hardest
The study pooled data from 287 population‑based studies, covering more than six million adults across 119 countries — one of the most comprehensive analyses ever conducted
Key regional findings include:
- Highest prevalence: Latin America, the Caribbean, and sub‑Saharan Africa
- Largest total number of adults with hypertension: East Asia and the Pacific, followed by South Asia
These patterns reflect both demographic shifts and systemic inequities in healthcare access.
The path forward
The researchers emphasise that the world does not need new miracle drugs or breakthrough technologies to reverse the hypertension epidemic. The solutions already exist — they simply aren’t being implemented at scale.
Evidence‑based strategies include:
- Affordable, widely available blood‑pressure medications
- Team‑based care models
- Accurate blood‑pressure measurement
- Simplified treatment protocols
- Health systems designed for long‑term chronic‑disease management
But these require political will, investment, and coordinated public‑health action.
Overall, this study is another stark reminder that lifestyle remains a cornerstone of hypertension prevention and control. Whole‑food, plant‑forward diets, regular movement, stress reduction, and reduced sodium intake are powerful tools.
But they must also be supported by systems that make healthy choices accessible, affordable, and sustainable. Hypertension is not just a medical issue; it is a societal one. And as this study makes clear, the world cannot afford another 20 years of slow progress.



{kind=link}