



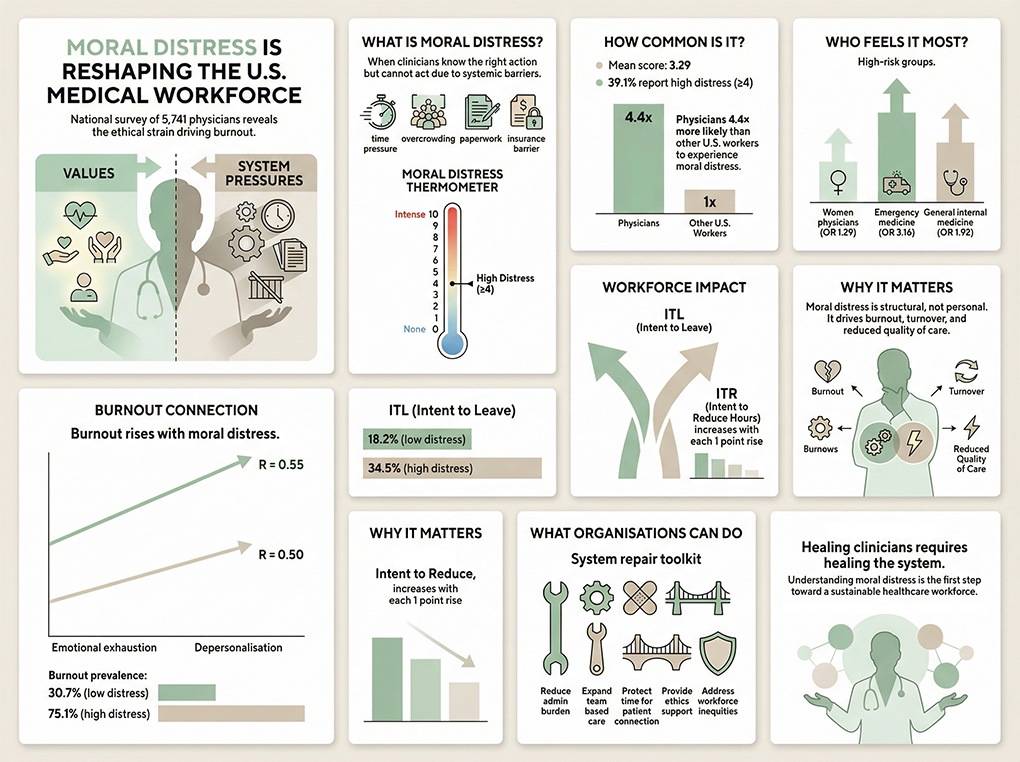
Burnout among US physicians has been described as a crisis, but new national data published in JAMA Network Open reveals a deeper, more insidious force driving that crisis – moral distress. It’s defined as the emotional and psychological strain that arises when clinicians know the right course of action for a patient but are unable to act due to systemic constraints.
This large cross‑sectional survey of more than 5,700 physicians and 3,500 U.S. workers offers one of the clearest pictures yet of how moral distress is shaping the modern medical workforce. The findings are sobering: moral distress is common, strongly linked to burnout, and significantly more prevalent among physicians than other US workers.
And the consequences ripple far beyond individual wellbeing—they affect patient care, workforce stability, and the long‑term sustainability of the healthcare system itself.
A national snapshot
The study surveyed physicians aged 29 to 65 across all specialities between late 2023 and early 2024. Using the Moral Distress Thermometer (MDT)—a validated 0–10 scale—researchers found:
- Mean moral distress score among physicians: 3.29
- 39.1% reported high moral distress (defined as ≥4)
- Physicians were 4.4 times more likely than other U.S. workers to experience moral distress
These numbers alone tell a powerful story: moral distress is not a fringe experience. It is woven into the daily fabric of clinical practice.
The study’s multivariable analysis revealed important patterns:
Women physicians
Women had 29% higher odds of experiencing moral distress than men. This aligns with broader evidence showing that women in medicine face disproportionate emotional labour, higher patient‑care expectations, and more systemic barriers.
Emergency medicine physicians
Emergency clinicians had over three times the odds of high moral distress compared with internal medicine subspecialists. This is unsurprising: emergency departments are ground zero for overcrowding, resource scarcity, and impossible trade‑offs.
Internal medicine physicians
These clinicians—often responsible for complex, chronically ill patients—had nearly double the odds of high moral distress.
Across the board, the pattern is clear: the more a speciality is exposed to system failures, the higher the moral distress.
The burnout connection
One of the most striking findings is the tight, graded correlation between moral distress and burnout.
Using the Maslach Burnout Inventory (MBI), researchers found:
- Emotional exhaustion and depersonalisation scores rose with every 1‑point increase in moral distress
- Correlation between emotional exhaustion and moral distress: R = 0.55
- Correlation between depersonalisation and moral distress: R = 0.50
These are strong associations in behavioural science—clear evidence that moral distress is not just a contributor to burnout, but a powerful driver.
The contrast between low and high moral distress groups is stark:
- 30.7% of physicians with low moral distress (<4) had burnout symptoms
- 75.1% of those with high moral distress (≥4) had burnout symptoms
That is a 2.5‑fold difference.
This is not about resilience. It is about the moral injury of being unable to practice medicine in alignment with one’s values.
The warning signs
Burnout is not just an emotional state—it is a predictor of workforce instability. The study found that moral distress is strongly associated with both:
- Intent to leave (ITL) one’s current position
- Intent to reduce (ITR) clinical hours
Again, the pattern is dose‑dependent:
- 18.2% of physicians with low moral distress intended to leave within 24 months
- 34.5% of those with high moral distress intended to leave
That is nearly double.
Given the existing physician shortage—and the projected shortfall of up to 124,000 physicians by 2034—these numbers should alarm every health system leader in the country.
Moral distress is not simply “stress.” It is the emotional fallout of being forced to act against one’s ethical compass. For physicians, this often means:
- Knowing a patient needs more time than the schedule allows
- Wanting to address nutrition, stress, or social determinants but lacking resources
- Being constrained by insurance rules or prior authorisations
- Witnessing preventable suffering due to system failures
- Feeling pressured to prioritise throughput over care
- Being unable to provide the standard of care one was trained to deliver
Over time, these experiences erode professional identity, compassion, and meaning—the very foundations of medical practice.
Systemic by nature
One of the most important implications of this study is that moral distress is not an individual failing. It is a structural issue.
The data show that:
- Moral distress is widespread
- It varies by speciality
- It correlates with systemic pressures
- It predicts burnout and workforce instability
This means that solutions must be organisational, not personal. Mindfulness apps and resilience workshops cannot fix a system that routinely forces clinicians into ethical compromise.
What Health Systems Can Do
The study’s authors emphasise the need to distinguish moral distress from burnout so that interventions can target the right problem. Based on the findings, effective strategies include:
1. Reduce administrative barriers
Streamline documentation, prior authorisations, and non‑clinical tasks that pull clinicians away from patient care.
2. Expand team‑based care
Integrate dietitians, social workers, mental health professionals, and health coaches to address root causes and reduce ethical conflict.
3. Protect time for meaningful patient interaction
Longer appointments allow clinicians to practice in alignment with their values.
4. Create mechanisms for ethical support
Regular debriefings, ethics consultations, and peer support groups can help clinicians process moral distress before it becomes burnout.
5. Address inequities in the workforce
Support women physicians and early‑career clinicians who face disproportionate burdens.
6. Align incentives with patient wellbeing
Shift from volume‑based to value‑based models that reward quality, prevention, and continuity.
A Call to Action
This national study makes one thing clear: moral distress is a defining feature of modern medical practice—and a major driver of burnout.
Physicians are not burning out because they lack resilience.
They are burning out because the system routinely places them in situations where they cannot provide the care they know their patients deserve.
If healthcare organisations want to retain their workforce, protect patient care, and build a sustainable future, they must address the ethical and structural roots of moral distress.
The soul of medicine depends on it.



{kind=link}